The most common brain tumors are metastases and malignant (e.g., astrocytomas) or benign (e.g., meningiomas, acoustic neuromas) primary tumors. Brain metastases occur in 5-10% of all adult patients with cancer and affect nearly 170,000 individuals in the US per year. Lung cancer is the most common primary source of brain metastases followed by breast cancer, unknown primary tumors and melanoma.1 Primary benign and malignant brain tumors are much less common than brain metastases with an estimated incidence rate of nearly 39,000 cases annually in the US.2
Surgery and chemotherapy have established roles in treating brain tumors, but for decades radiotherapy and radiosurgery have also been important tools in this area. The goals of radiosurgery are symptom relief, local tumor control, and potentially longer survival.3
Using the CyberKnife® system to treat brain lesions:
- Due to the high rates of recurrence of resected metastatic disease, surgical resection has often been followed by conventional radiotherapy. The CyberKnife® System has the advantage of effectively providing localized post surgical focused radiation treatment without the morbidity caused by conventional radiotherapy.3
- Non-isocentric radiation beam delivery (i.e., beams that do not have to converge on a single point) allows the dose distribution to conform to even irregularly shaped tumors.
- The accuracy of the CyberKnife® System has been shown to be sub-millimetric,4 allowing the delivery of large doses while avoiding critical structures.
- Frameless, non-invasive radiosurgery with the CyberKnife® System can be delivered in a single fraction or multiple fractions (sessions). This allows the dose to be spread over 2-5 sessions which may reduce the risk of damage to sensitive structures such as the cranial nerves and the eye.
- The safety and efficacy of the CyberKnife® System for the treatment of metastatic intracranial lesions is well established. Published reports indicate high rates of tumor control (91%) for intracranial tumor patients with low complication rates.3
- Benign intracranial tumors also can be effectively treated with the CyberKnife® System. A 98% tumor control rate and a 74% hearing preservation rate has been reported for 61 acoustic neuroma patients treated with the CyberKnife® between 1999 and 2001.5
- Patients with perioptic tumors have responded well to fractionated radiosurgery with the
- CyberKnife® System. High rates of tumor control (94%) and visual function preservation (94%) was reported in a series of 49 patients.6
Case I: Solitary Posterior Fossa Renal Cell Metastasis
(Courtesy Naples Community Hospital, Naples, FL)
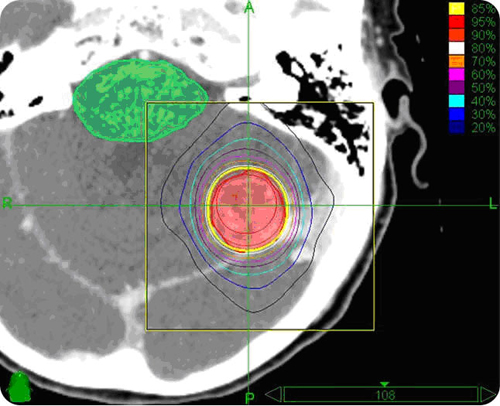
Axial planning image of a solitary renal cell metastasis to the posterior fossa showing the brainstem as a critical structure
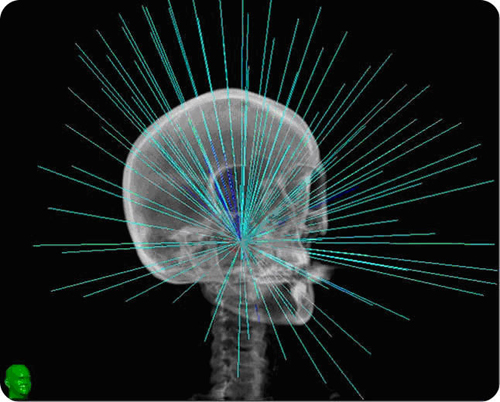
Right anterior oblique 3D image showing 90 CyberKnife® isocentric treatment positions and their relative intensities. The single fraction isocentric treatment in this case took 35 minutes.
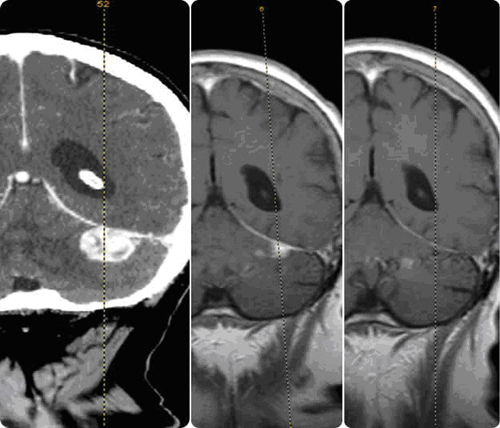
Comparison of pretreatment CT to 10 week and 16 week post-CyberKnife® treatment of a solitary renal cell metastasis to the posterior fossa. Tumor decreased to 18% of its original size at 10 weeks and was completely resolved based on MR six weeks later. Patient experienced nausea immediately following treatment which completely resolved.
Case 2: Optic Apparatus Meningioma
(Courtesy Barrow Neurological Institute / St. Joseph's Hospital and Medical Center, Phoenix, AZ)
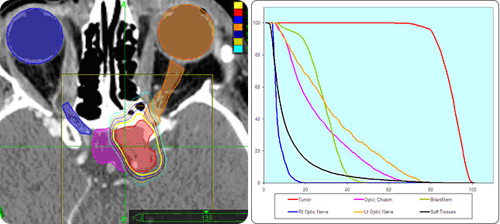
This female patient with a left optic apparatus meningioma which was jeopardizing vision to her remaining right-sighted eye chose the CyberKnife® System. Highly conformal treatment planning (left) optimized dose to the tumor and minimized dose to five critical structures surrounding the left optic apparatus. Tumor dose delivery and critical structure sparing is demonstrated by the DVH (right).
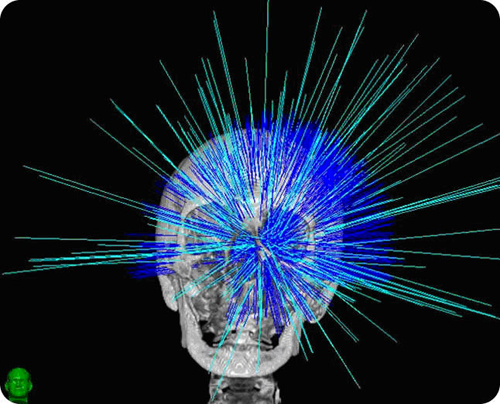
208 beam positions for the treatment of this optic apparatus meningioma demonstrates both the non-isocentric flexibility of the CyberKnife® System for treatment of the tumor. In this case the patient was treated with 5 fractions over 5 days at 40 minutes per fraction.
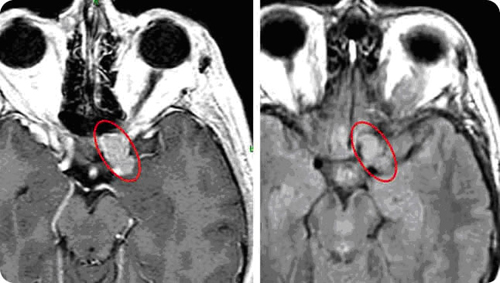
Prior to treatment, the vision in the patient's left eye was limited to shadow and light. Post-CyberKnife®treatment, the patient reported improvement in vision to her left eye. Pretreatment MR (left) and two months post-treatment MR (right) reveal that the mass is stable in size.
References
Khuntia D, Brown P, Li J, Mehta MP. Whole-brain radiotherapy in the management of brain metastasis. J Clin Oncol 2006;24(8):1295-304. PubMed ABSTRACT
Central Brain Tumor Registry of the United States, vol. 2006 Hinsdale, IL, 2006. LINK
Chang SD, Lee E, Sakamoto GT, Brown NP, Adler JR. Stereotactic radiosurgery in patients with multiple brain metastases. Neurosurgical Focus 2000;9(2):Article 7. PubMed ABSTRACT
Yu C, Main W, Taylor D, Kuduvalli G, Apuzzo ML, Adler JR, Jr. An anthropomorphic phantom study of the accuracy of CyberKnife® spinal radiosurgery. Neurosurgery 2004;55(5):1138-49. PubMed ABSTRACT
Chang SD, Gibbs IC, Sakamoto GT, Lee E, Oyelese A, Adler JR, Jr. Staged stereotactic irradiation for acoustic neuroma. Neurosurgery 2005;56(6):1254-61; discussion 61-3. PubMed ABSTRACT
Adler JR, Jr., Gibbs IC, Puataweepong P, Chang SD. Visual field preservation after multisession CyberKnife® radiosurgery for perioptic lesions. Neurosurgery 2006;59(2):244-54; discussion 44-54. PubMed ABSTRACT